
I’ve recently written a blog called ‘A patient’s understanding of pain’, which explains some of the difficulties I have found fitting my experience of persistent pain into some of the published models of pain. Armed with my new understanding of MY pain I decided to think through my approach to managing my persistent pain condition with a view to improving my situation going forward. This is the basis of this blog.
I don’t seek to repeat all the contents of my previous blog here, but to understand this current blog fully I suggest you read my ‘A patient’s understanding of pain’ blog first. It can be accessed by clicking HERE.
My persistent pain condition arises from a manual handling accident which took place around 10 years ago. I experienced a herniated disc which compressed my sciatic nerve. Around 18 months after the accident I underwent back surgery, but unfortunately my sciatic nerve was by then permanently damaged.
My sciatic nerve is sensitive and easily irritated. At the beginning of my pain journey I suffered severe back and severe neuropathic pain. I currently suffer with mainly neuropathic pain (at times severe) and some back pain.
Around four years after the accident I was lucky enough to have an episode of physiotherapy care undertaken by Consultant Physiotherapist Matt Low, based on a CFT approach. I have written about that episode of care HERE. Whilst working with Matt I developed my own visual approach to pain management which can be accessed HERE.
Although the basics of the pain management I developed at that time are still relevant to my situation now, I seek in this blog to reframe my pain management thinking to follow more closely my new understanding of my pain, based on the predictive processing model, with the hope it will enable me to further improve my situation.
My simple understanding of my pain
In my previous post ‘A patient’s understanding of pain’ I came up with the following simple understanding of my pain, based on the predictive processing model. I think this simple understanding works for both neuropathic and non-neuropathic pain, however I have chosen to centre it on my sciatic nerve pain as that is the prevalent difficulty for me.
I have in my mind/body a ‘model’ (predictive model) which I use to decide whether to give an experience of pain or not, in a variety of circumstances, based on presenting factors.
When a part of my body, in this case my damaged sciatic nerve (which may be being irritated by, for example, position, load or temperature), emits an ‘impulse’, then my predictive model considers this factor, along with other factors, to decide whether to give an experience of pain or not.
As well as the ‘impulse’ from the sciatic nerve, factors include my thoughts, feelings, beliefs, past experience with sciatic nerve, life experiences etc. Other factors might be, for example, environmental temperature, stress, tiredness and how irritated the nerve has been during the day.
My predictive model ‘knows’ what combination of factors are likely to be ‘ok’ and don’t need a response of pain.
If the combination of factors at that moment in time, including the ‘impulse’ from my sciatic nerve, matches the predictive model of being ‘ok’, then no action is taken, and no pain is produced.
If not, then pain is produced to alert me to do something to stop the irritation on the sciatic nerve continuing.
My predictive model changes with my experiences and is constantly being updated.
Understanding MY pain and developing a ‘narrative’ has been hugely important to me, but on its own this understanding isn’t enough to successfully manage my pain condition on a day to day basis. I need to use this understanding to seek ways to manage and improve my condition and continue to live as well as possible.
My pain management
In overall terms I view my pain management situation as needing to reduce the physical irritants on my sciatic nerve (of which unfortunately there are many), optimise as many personal, social, health and emotional factors and to consider, and hopefully address, any negative thoughts, beliefs and past experiences which might be acting as factors in my pain experience. As part of this I need to recognise, and hopefully improve, any negative pre-dispositions I have, such as anxiety, and build on my positive pre-dispositions, such as my resilience and having a naturally positive outlook.
The MindMap below gives a basic idea of when I get neuropathic pain, what physically makes it worse and what helps. Fundamentally though I have some pain all the time, but this is increased by standing still, walking a reasonable distance (for me), lifting and carrying and sitting. These activities particularly irritate my sciatic nerve. I am worse in the evenings as I experience ‘wind-up’ nerve pain. In addition to pain I experience numbness mainly in the lower leg and foot, which also varies depending on the activities I do.
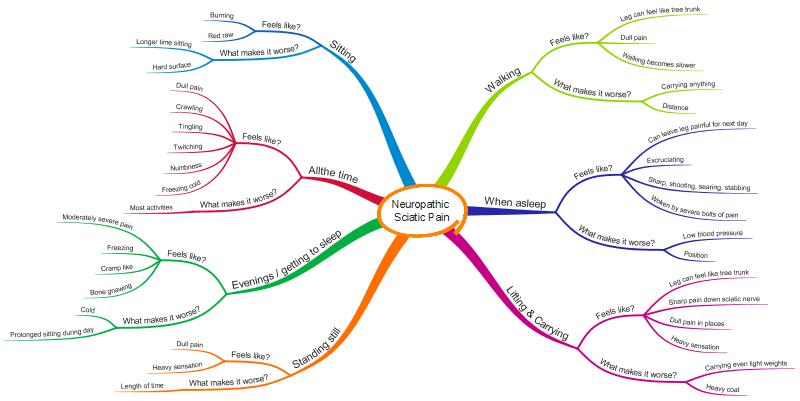
Unfortunately, you can’t tell from the MindMap how much pain I have, or how often I get each of the symptoms. I can’t yet think of an easy way to show this.
Thinking about the Predictive Processing model, and in particular ‘My simple understanding of my pain’, it is apparent that considering only what irritates my sciatic nerve is not going to optimise my pain management. There are far more factors involved in my pain experience than just what is physically happening to irritate my sciatic nerve.
I have therefore created the following MindMap, which focuses on me as a person, rather than just on my sciatic nerve. This MindMap highlights the areas that I think I need to attend to if I want to live as pain free a life as possible.
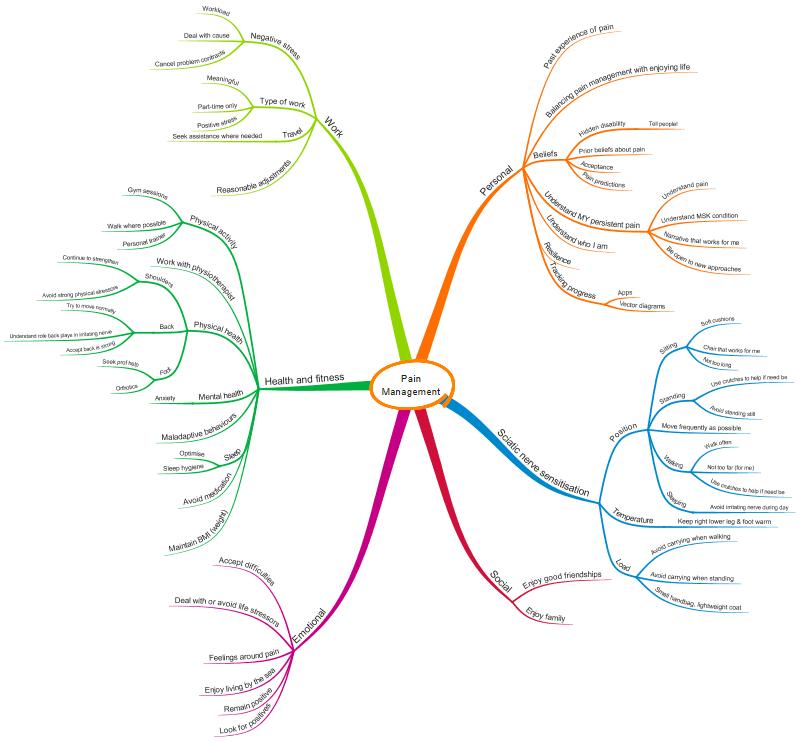
I’m sure you will find a lot of the factors on the MindMap obvious ones, such as stress, personal relationships, sleep, understanding pain, not lifting and carrying when I don’t need to, not sitting or standing for prolonged periods, using aids to assist me etc, but there are also some less obvious factors that undoubtedly impact on my pain experience, such as prior beliefs, conscious and subconscious predictions about what will cause me pain, past experiences, and thoughts and feelings around pain.
The MindMap is complex, reflecting the complexity of pain. There are some sciatic nerve specific elements, for example using soft cushions when sitting, understanding MSK conditions etc, but there are many elements that are more general, for example good sleep hygiene, enjoying good friendships and reducing anxiety. It is hard to address all these factors at the same time when trying to improve pain, and it is hard to work out whether the measures you are taking are having a positive impact on your pain, or not.
Tracking progress
I don’t always track my progress in terms of improvement (or otherwise) of my pain, but sometimes it can be useful. For example, when I first started to learn pain management and I was working hard on improving my pain situation, I tracked my progress using apps on my iphone.
I recently decided it would be helpful to track and measure my progress once more, but this time I decided to do it in a different way. My new tracking method, described below, is loosely based on work undertaken by my physiotherapist Matt Low around dispositions and on his use of vector diagrams. The following are Matt’s papers which served to inspire me.
A novel clinical framework: The use of dispositions in clinical practice. A person centred approach.
Managing complexity in musculoskeletal conditions: reflections from a physiotherapist
I know Matt, and possibly others, are currently working on developing dispositions and the use of vector diagrams, and I very much look forward to seeing how this work develops. Along with the predictive processing model I think this work has great potential to improve the lives of persistent pain sufferers.
I particularly like the idea of the vector diagrams in Matt’s papers as they provide an instant visual indicator of the extent of a difficulty.
There are numerous factors that combine in different ways at different times to give me a pain experience, but it wasn’t realistic to try and track them all. I decided to track the factors that I felt at the time were having the biggest impact on my pain experience, both positively and negatively.
I decided to split these factors into those that I felt were ‘pain contributors’ and those I felt were ‘pain improvers’. To improve my pain experience, I needed to work on decreasing the levels of these ‘pain contributors’ and increase the levels of the ‘pain improvers’.
Pain Contributors
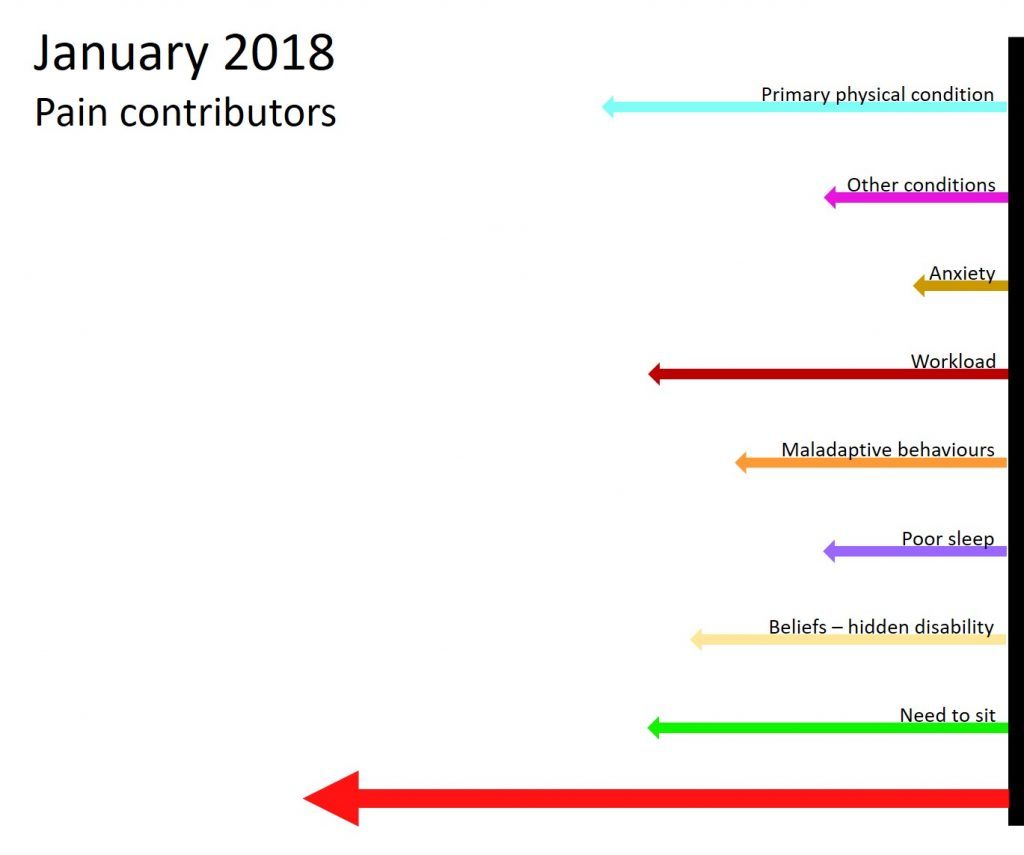
The following vector diagram shows the factors I identified as being the main contributors to my pain experience in January 2018. The length of the vector gives an indication of how big a problem I felt a difficulty was at that time.
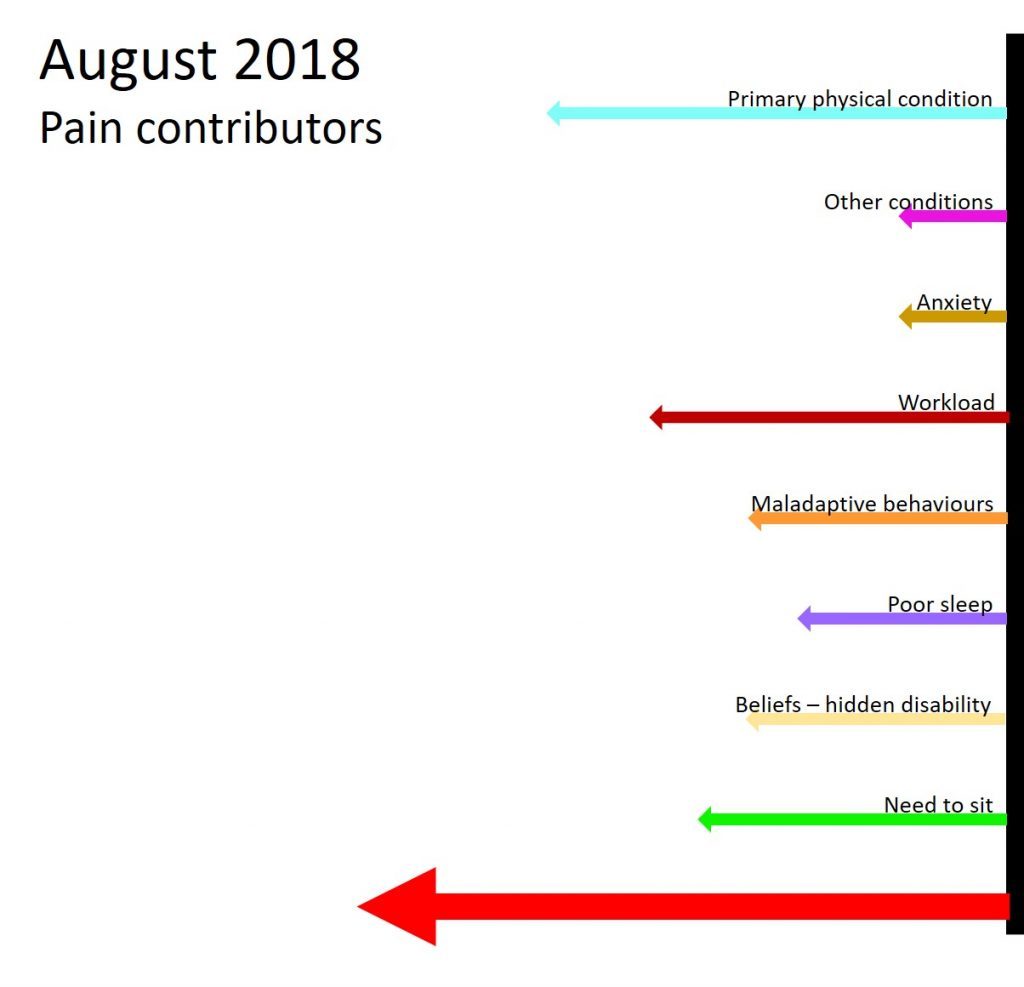
The next vector diagram shows how I rated the same factors in August 2018. You will see there are some elements I have been able to reduce, but some that have stayed static. The main improvements relate to my co-morbid physical conditions (foot bursitis, the remnants of shoulder impingement and a neck difficulty), my beliefs related to having a ‘hidden disability’, and my need to sit. There is a lot left to work on!
Pain improvers
The following vector diagram shows the factors I identified as being the main improvers of my pain experience in January 2018.
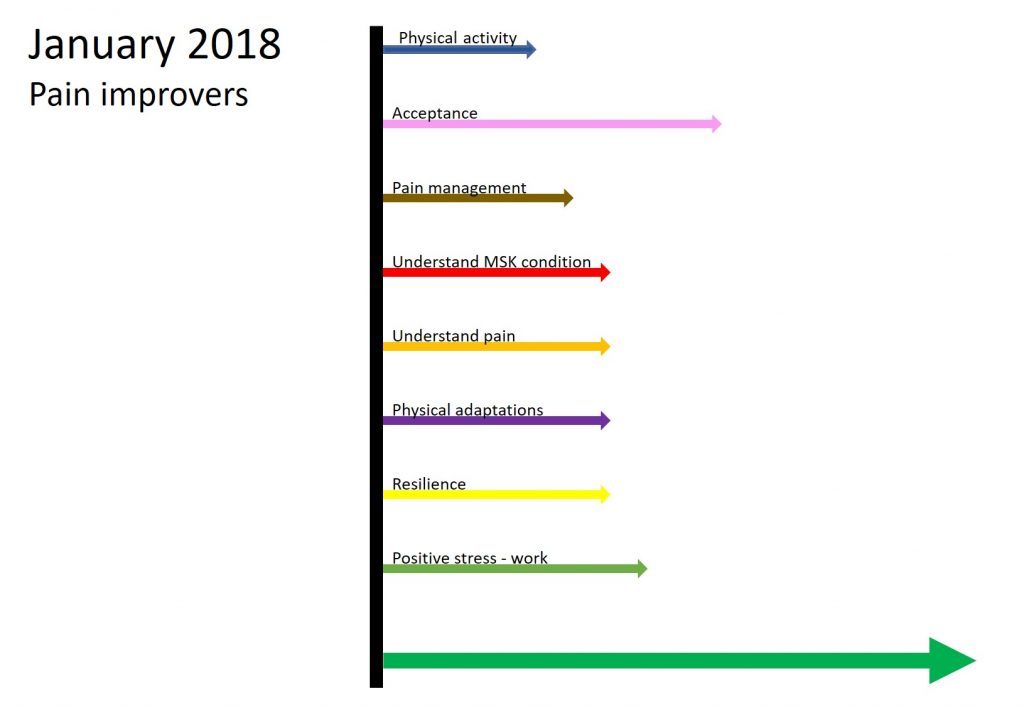
In my experience clinicians put more emphasis on negative pain factors, but I think it is helpful to put an equal emphasis on positive factors. After all, if you consider the predictive processing model then the positive factors play an important part in the experience of pain. I also think psychologically it is helpful to emphasise the positive as well as consider the negative. When you are in pain it is far too easy to focus on the negative. If you can try to focus more on positives, then I think this can really help you to take control of your situation and move forward.
The next vector diagram shows how I rated the same factors in August 2018. There are significant gains in physical activity, pain management, understanding MSK condition, understanding pain, physical adaptations and resilience.
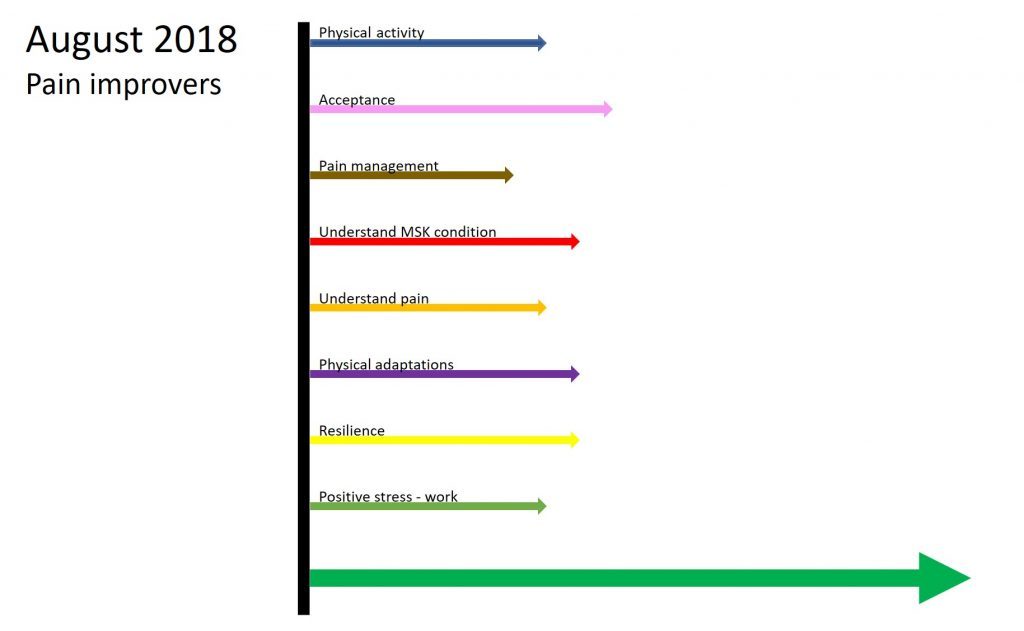
Overall, between January and August, it appears I was better at increasing the levels of ‘pain improvers’ than I was at decreasing the levels of ‘pain contributors’! More work to do!
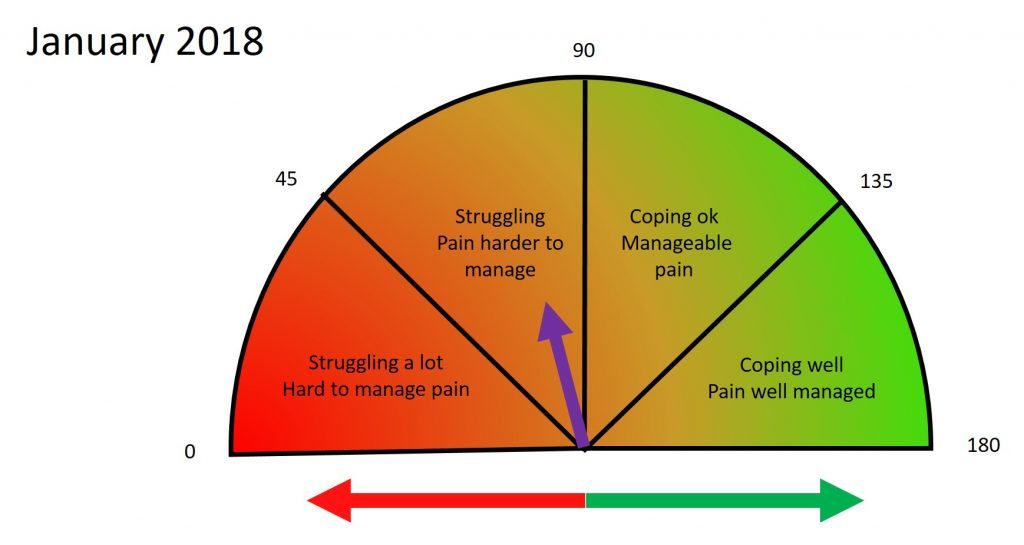
As well as tracking individual factors, I wanted to ‘see’ what improvement I had made in overall terms from January to August. I was particularly interested in my ability to ‘cope’ with my situation and the level of manageability of my pain. I therefore created the following ‘dial’ to show this. To be able to track progress using the dial I first needed to subjectively choose a starting point for where on the dial I felt I was in January. This is shown as a purple arrow. The green and red arrows relate to the ‘pain improvers’ and the ‘pain contributors’ diagrams above.
Using a bit of mathematical wizardry (well not that complicated really, just a few formulae), I converted the differences in the ‘pain contributor’ and ‘pain improver’ measures between January and August into a change of position on the dial, resulting in the diagram below.
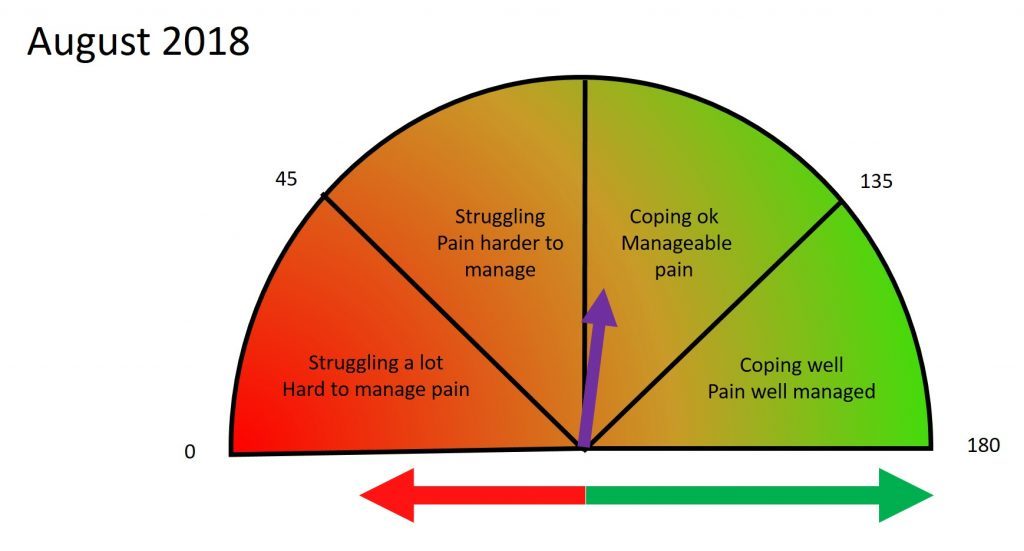
Comparison of the two dials shows a movement from ‘Struggling, Pain harder to manage.’ to ‘Coping ok, Manageable pain.’, which probably fairly reflected my overall situation. I found it helpful to ‘see’ that I had moved from a position of struggling, to one that I was coping better with. It is hard to explain, but even though I ‘knew’ my situation was improving, visually ‘seeing’ that was important to me. ‘Seeing’ it is somehow more tangible and reinforcing.
Although I appreciate this is not a conventional way of tracking pain, the use of vectors and the dial works well for me. I like identifying a small number of things to focus on, both positive and negative, and to measure them at different points in time using the length of a vector. I also like viewing my progress in terms of how I feel I’m managing my pain and how I feel I’m coping. Being able to track my progress in this way provides a level of positive reinforcement and encouragement.
Tina
@livingwellpain
www.livingwellpain.net



Well written, makes lots of sense and a big fan of visual ‘ dashboards’ for health improvements(or not….sometimes). A simple measure for pain increasing or decreasing does not take account the multiple contributors to pain.
Keep up the brilliant work you do, it provides hope to so many
X
Thank you so much Adrian.
Thank you for the information .
I have had lowerback pain after my car accident 2 years ago and I have been to almost every
doctor of middletown physical therapy and pain management.
My current doctor is http://comprehensivepainmanagement.us/ who I started
to see 4 months ago. He has given me medications and treatments
but also some physical exercises, which have help me alot in these 4 months.
I just hope the pain could completely go away.
Me too…. pain is difficult to live with, but not impossible by any means. Hope things go well for you 😊